Clinical AI can now be used against care teams, patients, and hospital systems. I’d boil this article down to one point: if your AI tools touch triage, meds, imaging, documentation, or patient messaging, you should treat them like a current safety and cyber risk today.
Here’s the short version:
- Prompt injection is already a working attack path. In one cited study, attacks succeeded in 94.4% of simulated clinical dialogues.
- Data poisoning can skew model behavior without obvious warning signs. The article notes even tiny data changes can hurt accuracy in high-risk use cases.
- Vendor AI adds extra risk. EHR add-ons, remote monitoring, imaging tools, and chatbots may change under the hood without clear notice.
- The impact goes beyond security. This can affect patient safety, HIPAA, bias review, downtime, billing, and care quality at the same time.
- The near-term fix is straightforward: keep an AI inventory, set ownership, test tools before launch, review third-party AI risk in more depth, log prompts and outputs, and have a rollback plan.
What stood out to me is that the threat isn’t just “bad answers from AI.” It’s hidden manipulation of inputs, training data, and connected systems that can make unsafe output look normal. That’s what makes this a hard problem for hospitals and health systems.
The Hidden Cybersecurity Risks When Doctors Use AI Diagnostics | Ep. 58
sbb-itb-535baee
Quick comparison
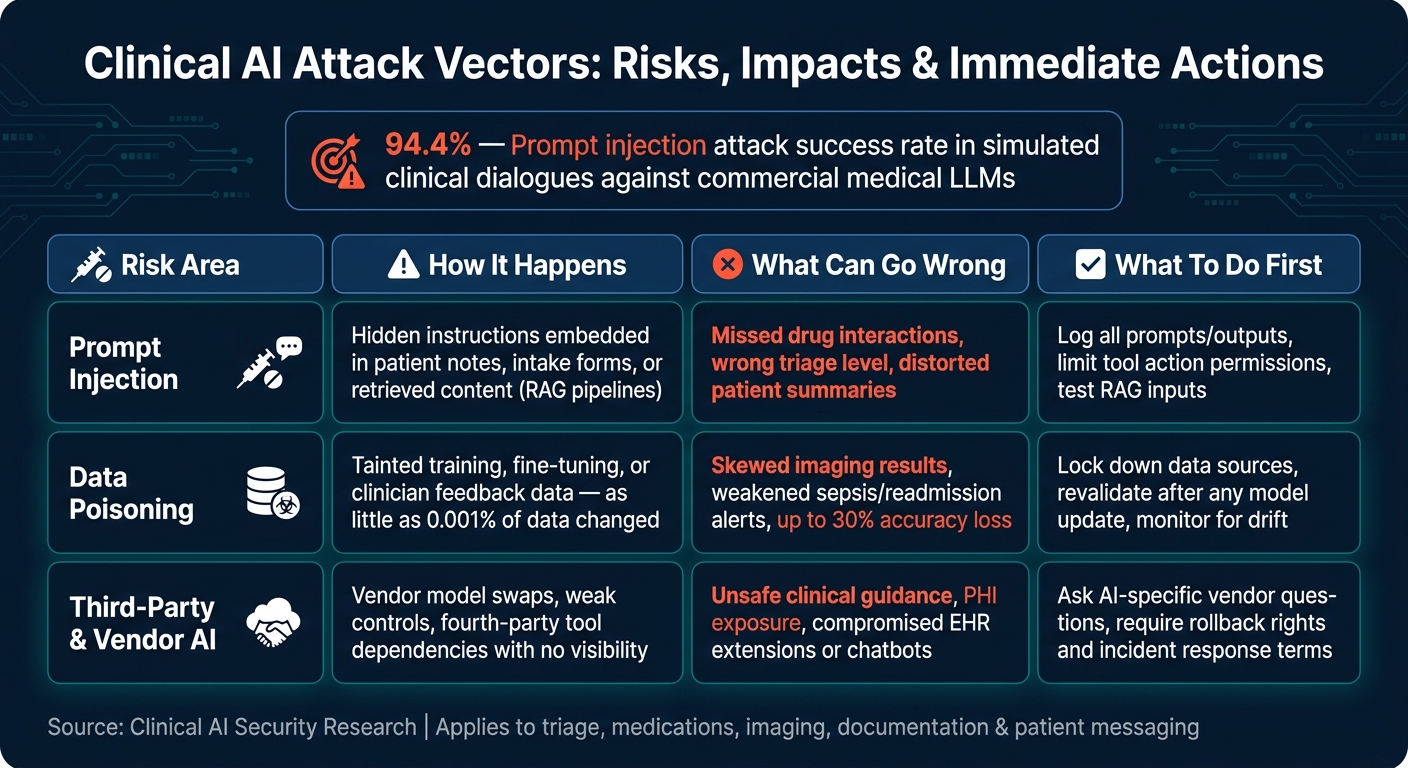
Clinical AI Attack Vectors: Risks, Impacts & Immediate Actions
| Risk area | How it happens | What can go wrong | What I’d do first |
|---|---|---|---|
| Prompt injection | Hidden instructions in notes, forms, or retrieved content | Missed drug interaction, wrong triage level, bad summaries | Log prompts/outputs, limit tool actions, test RAG inputs |
| Data poisoning | Tainted training, tuning, or feedback data | Skewed imaging, sepsis, or readmission outputs | Lock down data sources, revalidate after updates, watch drift |
| Third-party AI | Vendor model swaps, weak controls, fourth-party tools | Unsafe guidance, PHI exposure, weak oversight | Ask AI-specific vendor questions, require rollback and incident terms |
If I were leading security, IT, compliance, or risk on July 19, 2026, I’d read this article as a call to do three things now: govern AI use, test vendor tools like clinical systems, and prepare to shut off a bad model without breaking care workflows.
How attackers can exploit clinical AI in real workflows
Attackers can tamper with what clinical AI sees, learns from, or pulls into a response. The result can be unsafe output that still looks normal to a clinician. In day-to-day care settings, this risk tends to show up in prompt injection, data poisoning, and vendor-run AI tools.
Prompt injection against clinical copilots and AI assistants
Clinical copilots built into EHR workflows can draft referral letters, triage notes, and patient messages by pulling from notes, forms, and other retrieved content. Any one of those sources can contain hidden instructions that the model may follow.[3][8]
This gets more dangerous in retrieval-augmented generation, or RAG, pipelines. Why? Because the retrieved material may include patient-submitted forms or other outside content that an attacker controls.[3][8] A hidden instruction inside a patient intake form could tell the copilot to ignore a drug interaction, lower a triage priority, or write a summary that distorts the patient’s condition.
The risk gets sharper with agentic AI systems that can do things, not just write things. If a system can order tests, send messages, or update records, prompt injection can trigger actions nobody meant to approve - especially when tool access is too open.[3][8]
And it doesn’t stop with what the model reads in the moment. Attackers can also go after what the model learns from over time.
Data poisoning and model manipulation in diagnostic and risk models
Poisoning attacks contaminate the training, tuning, or feedback data a model learns from. That can slowly shift behavior, often without setting off alarms.[4][5] In practice, poisoned training data might cause an imaging model to miss tumors or weaken sepsis and readmission alerts.[4]
What makes this hard is that routine validation may not catch failures in small subgroups or rare cases.[4][11] Poisoning and backdoor attacks can leave top-line metrics looking almost the same while hurting accuracy in the places that matter most.[4][11] Research shows that changing as little as 0.001% of training data can cut model accuracy by up to 30% in safety-critical systems.[11] And attackers with access to only about 100 to 500 samples can still compromise AI systems.[10]
Retraining loops create another opening. If a model is updated based on clinician overrides or post-discharge outcomes, an attacker who can script automated feedback events may be able to mark harmful recommendations as successful. Over time, that can teach the model the wrong lesson and reinforce unsafe patterns.[4][5]
Third-party AI tools and connected technology as a clinical attack path
The risk goes well beyond models built inside the health system. Many providers depend on vendor AI for EHR extensions, remote monitoring platforms, imaging workflow tools, and patient-facing chatbots. Every product adds another path for attack, and health systems often have little visibility into how those vendor models work.[6][7][9]
There’s another problem here: vendors can swap models or change upstream components without making those changes easy to spot. The risk grows again when fourth-party dependencies enter the picture - for example, when a vendor’s AI depends on outside models or data sources the health system has never reviewed.[6][7][9] If a remote-monitoring tool or chatbot is compromised, it can feed unsafe guidance into routine care before staff catch on.[6][7][9]
PHI also turns this into a privacy issue, not just a safety one. HIPAA duties still apply when patient data goes into a third-party AI tool for inference or retraining.[6][9] A misconfigured or compromised vendor AI feature can spread unsafe decisions across the workflow with no clear warning signs.[6][9]
Why this threat is no longer theoretical
This risk has moved past the hypothetical stage because these attacks already work in clinical settings. Right now, not someday. The pattern is hard to ignore: attacks succeed, clinical AI is already in use, and the controls around it still trail behind.
Clinical adoption is outpacing AI-specific controls
Clinical AI is already built into EHR workflows. At the same time, governance, validation, and monitoring haven't kept up.
ECRI named insufficient AI governance a top health technology hazard.[15][16][17] That warning goes beyond standard IT headaches and straight into patient care. When these tools sit inside care delivery, a failure isn't just a software bug anymore. It becomes a clinical event.
Patient safety, compliance, and operations are all at risk
The risk shows up in patient safety first. FDA MAUDE identified 43 harm incidents tied to machine-learning medical devices, including radiation overdoses and mis-targeted radiotherapy.[17] An academic review also found that a sepsis algorithm used at hundreds of hospitals missed sepsis cases and flooded clinicians with alerts.[17]
Research findings add another layer of concern. Prompt injection attacks against commercial medical LLMs succeeded in 94.4% of simulated clinical dialogues, including cases involving contraindicated medications in pregnancy and dangerous drug interactions.[12][18] Those aren't edge cases. They're the kinds of situations clinicians deal with every day.
Compliance risk is climbing too. HHS/OCR's Section 1557 guidance requires organizations to identify and mitigate discriminatory AI outputs.[13] Proposed HIPAA Security Rule updates would also include AI systems in formal risk analysis.[14]
That means AI-specific governance, validation, and response controls are needed now.
What healthcare leaders should do now
AI oversight can't be a one-and-done task. It has to stay in motion: governance, vendor control, and monitoring. In practice, that means your controls need to cover approval, vendor intake, and what happens after launch.
Build AI governance, ownership, and approval controls
Set up a cross-functional AI governance committee, led by the CIO, CISO, or Chief Digital/Clinical Officer. Have it meet quarterly, keep the AI inventory up to date, and define approval criteria for the same attack surfaces covered earlier: prompts, training data, and third-party tools.[19]
Track every AI and ML tool used across clinical, billing, scheduling, population health, and revenue cycle workflows. Give each one a risk tier. For high-risk use cases like medication changes, triage, and radiology prioritization, require human review.
Before anything goes live, get sign-off from clinical, security, privacy, legal, compliance, procurement, and operations. Document the model's purpose, limits, training data sources, subgroup performance, monitoring plans, and rollback procedures. At least once a year, bring the board a summary of high-risk use cases, incidents, and key metrics.[19]
Add AI-specific vendor due diligence and validation testing
Standard security questionnaires don't cut it for clinical AI. If you want to deal with the prompt injection and poisoning risks covered earlier, ask vendors direct questions:
- How do you prevent prompt injection, prompt-based data exfiltration, and jailbreaking?
- How do you control training and fine-tuning data?
- Can you roll back to an earlier version after a bad update?
- Can you provide subgroup performance data by age, sex, race/ethnicity, and relevant comorbidities, not just top-line accuracy?
- Do you have written proof of independent penetration testing and a documented incident response plan?
Then test the model against retrospective or synthetic data from your own patient population. After that, run a 30- to 90-day shadow-mode pilot that logs recommendations and compares them with actual clinical decisions. Set launch criteria in advance, and require sign-off from clinical, security, and compliance before access expands. Once the model is deployed, revalidate it whenever the model changes, the EHR goes through a major change, or your patient population shifts.
Set up monitoring and incident response for AI failures
After launch, the focus changes. It's less about approval and more about drift detection and fast containment. On the technical side, track input and output distributions over time so you can spot performance drift. Log prompts and outputs to catch unsafe responses. Alert on unusual prompt patterns that may point to injection attempts. On the clinical side, watch override rates - how often clinicians reject AI recommendations - and flag unusual spikes by unit or provider.
Make sure SIEM, SOC, and safety reporting tools can flag AI-specific incidents and send them to reviewers who know what they're looking at.
When an incident happens, speed matters. Disable the affected feature, roll back to an earlier model version, or shift to manual fallback workflows. Check patient impact right away, with close attention to high-risk areas like medication management and emergency triage. Preserve logs of prompts, outputs, model versions, and system events before anything gets overwritten. Bring in the vendor within the timeframes set in the contract, and involve privacy and compliance to decide whether HIPAA breach notification rules apply. Each incident should feed back into governance, vendor requirements, and monitoring thresholds.
Conclusion: Treat clinical AI exploitation as a current risk, not a future scenario
Prompt injection can take over clinical copilots. In controlled research, it led to unsafe or contraindicated recommendations 94.4% of the time.[2] Data poisoning can also damage diagnostic models for 6 to 12 months or longer before anyone spots the issue.[1][20] And third-party AI tools used in imaging, documentation, and triage open indirect paths into care delivery that many security programs don't catch.[21]
That risk doesn't stop at IT. It hits patient safety, daily operations, and compliance all at once. The fallout can include delayed diagnoses, missed alerts, inappropriate treatment, disrupted scheduling, imaging slowdowns, billing errors, HIPAA exposure, and FDA software-as-a-medical-device concerns.
The response has to match the attack surface. In plain English, that means clear governance and clear ownership. It also means third-party vendor risk management for AI, pre-deployment validation, and incident response processes that can isolate a compromised AI feature without taking down the clinical workflow around it. Waiting to deal with this later leaves organizations exposed right now.
How Censinet supports AI risk management at scale
Making those controls work at scale takes shared workflows, consistent risk data, and fast routing of findings. Teams need to keep track of AI tools, coordinate approvals, run vendor assessments, monitor open risks, and keep governance records up to date. Censinet RiskOps™ brings those workflows into one platform, so security, compliance, clinical, and procurement teams can see where AI is in use, which risks remain open, and what actions still need attention.
Censinet AI helps speed third-party assessment with AI questionnaires, evidence summarization, and vendor risk scoring. That lets teams review vendors more efficiently while keeping clinical safety in view. Censinet AI™ also supports orchestration across GRC teams by routing findings and tasks to the right reviewers and helping maintain human-guided oversight. Human decision-makers still handle approval, risk acceptance, and incident authority; Censinet provides the workflow and data needed to scale that oversight.
FAQs
How can clinicians spot AI manipulation early?
Clinicians can catch early AI manipulation by paying attention to behavior that falls outside normal clinical patterns, even when standard security alerts stay quiet.
A few signs tend to stand out. One is inconsistent model behavior across patient groups or facilities when there’s no clear clinical reason for the gap. Another is unexplained performance drift after retraining. Data workflow issues can also hint that something’s off, such as sudden shifts in lab value distributions or spikes in late electronic health record edits.
Which clinical AI tools should be reviewed first?
Prioritize AI tools that access PHI or shape clinical decision-making. That includes sepsis prediction models, radiology image classifiers, ECG interpretation algorithms, and AI-assisted differential diagnosis systems.
These tools touch patient safety and diagnostics head-on, so they need deeper validation for intended use, subgroup performance, and clinical risk. In plain terms, the stakes are higher, so the review has to be tougher.
Classify every AI tool by safety impact, and give high-risk systems the strictest scrutiny.
What should a hospital do after an AI incident?
Treat the incident like any clinical safety event: identify the problem fast, cut risk, and protect patients from harm. The response should use a patient-safety-first framework, not just standard software procedures.
Keep clear incident playbooks that line up with HIPAA and other regulatory rules. Those playbooks should include forensic analysis, documented rollback steps, and clear thresholds for shutting down affected AI systems and switching back to manual clinical workflows.
